Molecular analysis of Omicron variant shows it's 'highly evasive of immunity': UBC
Source: Coast Mountain News (British Columbia)
Molecular analysis of Omicron variant shows it’s ‘highly evasive of immunity’: UBC
Vaccines remain the best defence, researchers found
KATYA SLEPIANDec. 22, 2021 8:50 a.m.NEWS
A group of University of B.C. scientists have unveiled a molecular-level analysis of the Omicron variant that is swiftly becoming the dominant strain of COVID-19.
The analysis, which was done at “near atomic resolution” using a cryo-electron microscope, showed how the heavily mutated variant infects cells and is “highly evasive of immunity.”
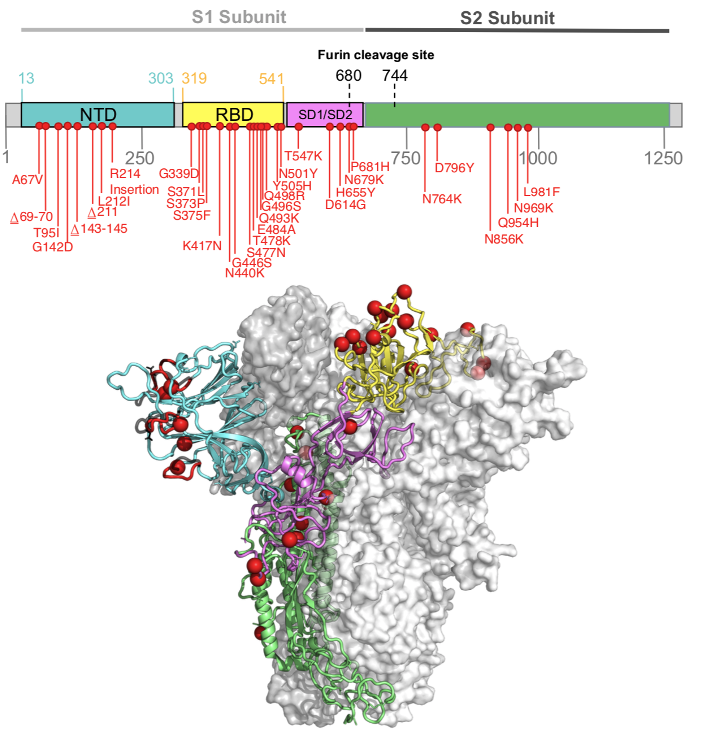
Sriram Subramaniam, a professor at UBC’s faculty of medicine’s department of biochemistry and molecular biology, said that the Omicron variant had 37 spike protein mutations, much more than any previous variants.
According to Subramaniam, that has big implications for how the variant will act, because the spike protein is responsible for both how the virus attaches to and infects human cells and because its also where the antibodies attach to fight off the virus.
Read more: https://www.coastmountainnews.com/news/molecular-analysis-of-omicron-variant-shows-its-highly-evasive-of-immunity-ubc/
Picture of the enemy:

 = new reply since forum marked as read
Highlight:
NoneDon't highlight anything
5 newestHighlight 5 most recent replies
= new reply since forum marked as read
Highlight:
NoneDon't highlight anything
5 newestHighlight 5 most recent replies

Just_Vote_Dem
(3,736 posts)Unfortunately for us

Aussie105
(8,368 posts)The virus is outsmarting the human race.
With millions around the world incubating the virus and providing a rich ground for further mutations, this virus isn't going away at any time soon.
Maybe, in 10 years time, the survivors may look back and say . . . If Only!
Not while there are unvaccinated people, not while governments around the world want their economy kept bubbling long bu not having lockdowns.

paleotn
(23,106 posts)We've known how to deal with infectious disease for centuries. It's not terribly complicated. It's simply a matter of will. We chose not to. And not just the Trump administration. Nation states around the globe chose to allow this pathogen to become endemic in human populations. Now we reap the whirlwind.

wnylib
(26,875 posts)that keeps it active.
I read that earlier, but how the he!! does the deer population get it? Hunters? water supply?
Here in PA, they said some 30% of the deer test positive (unless it's found through PCR with high rates and it's really another similar virus?)
orangecrush
(31,932 posts)
GB_RN
(3,602 posts)In fact, it's about as far from good news as you can get in terms of virology. Even if it's less lethal than Delta (and Omicron's lethality hasn't been established yet), the fact that it spreads so quickly, it will overwhelm the hospital systems and cause deaths when people can't get medical care.
paleotn
(23,106 posts)Normal morbidities aren't going to take time off for this covid thing. God help those with heart attacks, strokes or car wrecks. 
Orrex
(67,565 posts)While we're at it, companies should abandon the work-from-home model and bring their valued employees back into their poorly ventilated and minimally sanitized offices, because ideas might be exchanged or something.
Aussie105
(8,368 posts)From the politicians anyway. Unified cries of 'The Economy!' and 'The supply Chain!'
Medical staff in hospitals would not agree.
wnylib
(26,875 posts)will collapse.

BumRushDaShow
(173,850 posts)They uploaded their paper for peer-review - https://www.medrxiv.org/content/10.1101/2021.12.19.21268028v1
Link to tweet
@Tuliodna
·
Dec 18, 2021
Replying to @Tuliodna
In Nov 2021, genomic surveillance teams in South Africa & Botswana detected a new SARS-CoV-2 variant associated with a rapid resurgence of infections. Within 3 days, it was designated a variant of concern (Omicron) by @WHO and, within 3 weeks, had been identified in 87 countries.
Image
Tulio de Oliveira
@Tuliodna
The Omicron variant is exceptional for carrying over 30 mutations in the spike glycoprotein, predicted to influence antibody neutralization and spike function.
Image
2:44 PM · Dec 18, 2021
wnylib
(26,875 posts)about omicron. If it evades antibodies so well, and resists antiviral meds, how can it also be less lethal than delta? Less lethal means that the immune system can fight it and recover. So how does that happen if omicron is resistant to antibodies? Is it more vulnerable to other parts of the immune system?
BumRushDaShow
(173,850 posts)is that apparently because of the new configuration of the spikes, the change slightly alters where the viral particles have tended to "land" and the way they fold around (like jello strands), it can make it difficult for the immune cells to get to the viral spikes or virus body itself, then attach, and then start neutralizing it.
In general with these variants, they find cells that have certain "receptors" (ACE2) and then like velcro, the virus can attach to those locations, puncture the cell wall, and then inject their genetic material in it to start replicating.
A computer sim of the virus is here (you can see the "spikes" with the cluster of stuff at the end, which was from a Nature article here - https://www.nature.com/articles/d41586-021-02039-y) -

The fascinating illustration of how they attach and pull in to the cell -

The (landing) receptors are located all around the human body on some critical organs like the lungs (most common), heart, kidneys, and even along the neural, digestive, and circulatory systems. The entry points (nose/mouth) have quite a few so the virus can land there first and start reproducing, and then those child viral particles can move deeper into the body.
However what they are finding is that based on the changed configuration of the Omicron spikes, there have been some more favorable landing zones along the way to the lungs (bronchial tubes) that are not as deep inside them and that has apparently lessened the more immediate severe impacts in the lungs. I.e., they were finding that this version of the virus, if it makes it deeper inside the lungs, is apparently slower to find a place to land and reproduce.
December 15, 20217:15 PM ET
Michaeleen Doucleff 2016
Omicron is spreading lightning fast. In the U.S., the percentage of cases caused by this new coronavirus variant jumped seven times in just a week, from 0.4% of the total cases sequenced to 2.9%, the Centers for Disease Control and Prevention estimates. And it's already causing about 13% of cases in a region that includes New York and New Jersey.
In a household, the risk of spreading the omicron variant to another member is three times higher than it is with the delta variant, U.K. health officials estimated Friday. And delta, as you may know, is considered highly transmissible. Why is omicron such a superspreading variant? Preliminary data, published online Wednesday, gives us the first look at how omicron may behave inside the respiratory tract — and the data offers a tantalizing clue as to why this heavily mutated variant is spreading so fast and even outcompeting delta.
The omicron variant multiplies about 70 times faster inside human respiratory tract tissue than the delta variant does, scientists at the University of Hong Kong report. The variant also reaches higher levels in the tissue, compared with delta, 48 hours after infection. "That's amazing," says immunologist Wilfredo Garcia-Beltran, who's a fellow at the Ragon Institute of Massachusetts General Hospital and wasn't involved in the study. This finding indicates that mutations in omicron have sped up the process of entering or replicating (or both) inside the tissue.
But how this finding, from tissue studied in the lab, relates to viral loads inside an actual person's respiratory tract is still unknown, he emphasizes. These findings from the University of Hong Kong haven't been peer reviewed — and the experiments occurred entirely inside cell tissue. Nonetheless, the research supports another study, published online Tuesday, from Garcia-Beltran and his colleagues that also suggests omicron is more infectious than delta.
(snip)
https://www.npr.org/sections/goatsandsoda/2021/12/15/1064597592/a-tantalizing-clue-to-why-omicron-is-spreading-so-quickly
The research above was based on in vitro (in the lab) behavior of the virus with lung tissue and bronchial tissue vs actual observed behavior in vivo (in the body), but it gives some clues that can be further looked at.
One of the things that a number of not just viruses but bacteria can do, is configure themselves to make it harder for the various cells that make up our immune system (and there are a number of them) to find a place to attach to them and neutralize them.
In general the body has many actors that have certain roles when an infection occurs - some that react immediately and others that eventually adapt to help join the fight. It's like an army with various specialists.

In the above circle of entities to the left, you have the "first line of defense" that get triggered with an infection and then those seen in the circle to the right, are what make up the final attack response to an invader, and can be enhanced by vaccines.
(sorry I geeked out on you but as a former chemist, I couldn't help it
 )
)YP_Yooper
(291 posts)Thank you so much for real science! I had to go and read the whole article, and bookmarked it with the others. As a former chem eng, I love this stuff. To me, this is science, not the far too many headlines telling us what science is from reporters and politicians 
BumRushDaShow
(173,850 posts)I used to be in chem and physics classes with ChemEs and pre-meds.
I never really thought of myself as a "visual" learner but over the years, stuff like this has pointed to how I apparently am. It's like remembering when taking multivariable calculus and how my old professor would say it was nothing more than taking 2-dimensional curves and rotating them around a 3rd axis to get a volume. I was like whoa! 
And as another visualization to add (I didn't want to completely swamp the previous post) - this shows just how the thing enters a cell, reproduces, and exits (I think from the same article) -

The one thing that lay folks have to realize is how tiny viruses are compared to the cells they break into (and that even includes bacteria, which are also larger than viruses).

wnylib
(26,875 posts)As long as the terminology is not too specialized, I can follow the process being described.
The bronchial infection by omicron concerns me very much because I am highly vulnerable to viral bronchitis. Every common cold or ordinary flu becomes viral bronchitis in me shortly after I get infected. Once I have bronchitis, I get multiple asthmatic attacks a day from reactions to the virus.
An allergist told me that my asthma and chronic chest congestion from multiple allergies provides a good breeding ground for viruses. He advised me to use antihistamines during cold and flu season to cut back my vulnerability to bronchial infections. It works for ordinary flu and common cold. But don't antihistamines work by suppressing the immune response? Isn't it risky to do that in a viral pandemic?
I am concerned that, although omicron is mild for most people, it would be much worse for me because of my high susceptibility to bronchial infections.
Are people with multiple allergies more prone to cytokine storms because of the immune response overreaction in allergic people? There are 4 substances that can produce anaphylactic reactions in me and it has happened to me twice.
So isn't omicron more risky for people like me?
YP_Yooper
(291 posts)My wife is similar. You're correct about the steroidal inhalers - they can suppress the immune system (but if it's necessary to breathe, well, stuck using it, I guess). However inhalers like Advair was found to help with dilation without the effect steroids do, and had a side benefit of inhibiting the replication of the virus. We all had COVID last month, and her coughing was pretty frequent, she came though after about 5 days pretty well using Advair first, inhaler if needed.
Antihistamines may suppress the immune system to some extent, but because the body's response to COVID is one of inflammation, it may help more than hurt. May also add that it looks like Omicron loves your sinuses, and if you're vacc'd or had it before, doesn't do well at all in your lungs and the rest of your innards, so another plus.
Hope you don't ever need to find out personally
BumRushDaShow
(173,850 posts)after potentially having contracted swine flu (at the tail end of it in 2010) and getting pneumonia from it and that stuff was $250/month. 
My pulmonologist wanted to keep me on it forever (I was like um no... ). I never had continual "chronic" bronchial issues to justify it. It was always more something that got triggered and would resolve.
I expect something like Advair (or equivalents - it finally generic versions) might be useful for anyone that ends up with long COVID if there was more severe lung damage that has been slow to heal.
BumRushDaShow
(173,850 posts)although much of it may have been reaction to bacteria more than viral. Still I kept either Bronkaid Mist or Primatene Mist (both recently reformulated and reintrodcued after removing the CFCs) - all before my PCP gave me an albuterol script. I prefer the epinephrine though but haven't needed it anymore as my triggers (at one time pet dander allergies and some other things) have resolved as I aged.
I don't know how allergies impact cytokine storms though, although any respiratory virus, including flu, can really impact those who do get chronic bronchial infections... I know I ended up in the hospital with pneumonia at the tail end of the last swine flu outbreak in 2009/2010, which triggered an exacerbation, and was on IV steroids (prednisolone) and oral prednisone.
wnylib
(26,875 posts)viral bronchitis, I had 4 bouts of it in one winter due to a coworker who kept infecting everyone because she refused to get treatment until HR told her to see her doctor or stay home.
Z-pak and Albuterol inhaler worked well for me each time I got re-infected. But, since I was over 60 at the time I developed a viral aftermath that affects primarily people 60 and over with north European ancestry, polymyalgia rheumatica - a muscle and joint inflammation. It was very painful and crippling.
By the time the PMR was correctly diagnosed and treated, it took two years of Prednisone and exercises prescribed by a rheumatologist to recover full range of motion. When I hear descriptions of long covid muscle inflammation, it sounds a lot like what I went through with a long term effect from a viral infection.
So the high contagion and bronchial infection of omicron has me concerned.
YP_Yooper
(291 posts)but from what I've read, 2 reasons:
1) it simply replicates much faster in the sinuses, where antibody response is quite different - like a separate, first response immune system (mucosal immune system) different from the antibodies in your blood that are developed from vaccines.
2) it has a harder time infecting the lungs where your typical conversation about vaccine induced antibody response comes in.
Since it's a wildfire in the sinuses, it's far easier to get out of your head and into the air to get the next person. A vaccine induced antibody response protects your lungs and the rest of you from severe disease (since that's where the antibodies are) while your mucosal immune system learns to identify Omicron and kills it off, also developing a stronger protective response in your mucosal system - in addition to the "internal" antibodies you have.
If you're really bored, or just interested:
Immunobiology: The Immune System in Health and Disease. 5th edition.
https://www.ncbi.nlm.nih.gov/books/NBK27169/

moriah
(8,312 posts)The data is still limited, and I don't think we'll know for a month exactly how Omicron acts in a lower-vaxxed area of a medicalized nation. I can wish that it will be less lethal for those who are unvaccinated -- we simply won't know, especially for the older unvaccinated population, for three weeks to a month.
However, it's presumed that the known human coronaviruses that still circulate among humans as "colds" each first started as something like this emergence into the human population -- it's more beneficial to them continuing to circulate in us to not cause us as severe of disease. Otherwise we stay home in bed instead of sneezing all over work.
By causing such severe disease and so many ICU admissions/need for ventilators, it shows in a way that the original COVID-19 was not a very evolved virus. The original virus didn't spread as fast to areas with less concentrated populations -- but Beta did, and Delta even faster. If current infections are trending to be Omicron even in my state of Arkansas (which we won't be told) now, it's going to be three weeks to a month before we really see if ICU admissions and particularly vents stay low compared to hospitalizations.
My state has plenty of beds to create standard wards to treat people who don't need ICU or vents. We do NOT have the ICU capacity, though, to handle what could happen if it overtaking Delta will mean a huge bloom in cases again here in states like Arkansas -- or worse, a larger bloom than the ones we had with Beta and Delta because it transmits more easily without needing to be in a large city/as crowded of a population.
For COVID to mutate into a virus that causes a cold instead of viral pneumonia it may take a successive number of weaker but more transmissible variants to emerge. Whether Omicron is truly the first step towards that is still a question.
But we can hope it is, for all the people who can't get a shot. Even if those having to give us our data about that are those that have chosen not to get vaccinated when people where it's not available easily would love to have free shots available to all.
monkeyman1
(5,109 posts)
IronLionZion
(51,722 posts)Terminate with extreme prejudice
This is what the enemy pics look like to me


SunSeeker
(58,444 posts)flying_wahini
(8,284 posts)Heart failure rate from Omicron is increasing quickly…
https://vm.tiktok.com/TTPd6L92oe/
(Just posted this earlier…)
YP_Yooper
(291 posts)but anecdotal from one doctor who "knows" it's from Omicron
At the risk of a flame war (and this is not at all intended as anti-vacc, just understanding the numbers science), it may also be from the booster shots as well. From the NEJM talking about the rate of myocarditis (heart issues like the doc mentions) just the initial 2 shots, not including a 3rd booster magnifying the effect. This was also backed up by Pfizer's emergency authorization research:
As an example, "Among all the patients between the ages of 16 and 29 years, the incidence per 100,000 persons was 5.49 (95% CI, 3.59 to 7.39)"
https://www.nejm.org/doi/full/10.1056/NEJMoa2110737
It's a numbers game. In NYC with a population of 9M, one would expect 500 or so cases at least just from the vacc, not including those anti-vacc who got infected. With around 1900 total beds across the area (may be dated on this one) servicing all the needs of the city, one can see how this could be impacting the good doctor.
Also noted that this doesn't mean death, but a condition (mostly manifesting itself as chest pains) that would need hospital care, and generally resolves itself on its' own in 50% of those cases.
nowforever
(586 posts)One of theories is that viruses evolved from a primitive cell that had a nucleus several billions years ago. They are thus highly evolved with an intelligence to exist without really living...very clever. Entire plant and animal populations have become extinct due to viruses.

Deminpenn
(17,640 posts)If it is true, then hospitalizations and deaths should be showing the same vertical spike as case numbers, assuming the new cases are nearly caused by the latest mutation. Except neither hospitalizations nor deaths are.
The latest mutation may be better at evading vaccine derived immunity, but I doubt it is evading the entire human immune system.

OverBurn
(1,292 posts)A virus of some type is what is likely to wipe out the human race some day. It's obvious we will not be smart enough to save yourselfs.