2016 Postmortem
Related: About this forumThe Best Health Care Fix You've Never Heard Of
We should listen to Martin O'Malley on all-payer reform.
'There was a moment in the second Democratic presidential debate that perfectly illustrated the difficulty of dislodging the media’s comfortable narratives. The topic was health care, and Hillary Clinton and Bernie Sanders lined up in their familiar positions: Clinton defending Obamacare and citing ways to improve it, Sanders supporting a national single-payer plan to guarantee health care as a right and not a privilege. These are the two dominant poles on the Democratic side: building upon Obamacare, or simply overhauling it.
And then Martin O’Malley tried to chime in.
“I really wish you’d come back to me on this on, John,” said the former Maryland governor to moderator John Dickerson. “Because we have found a way to reduce hospital costs, so whenever we come …”
But CBS wanted to go to commercial, so Dickerson replied, “Governor, you’re breaking the rules.”
Dickerson was talking about pre-arranged debate rules against interruption, but he might as well have been talking about the media’s unwritten rule that there can only be two sides to any issue, any question, at any particular time. That’s a shame, because O’Malley actually did employ an obscure yet worthwhile “way to reduce hospital costs” during his governorship, and it’s no small matter. It threads the needle between defending Obamacare and abandoning it, between today’s technocratic system and tomorrow’s vision for national health care. It’s called all-payer rate setting.
The best way to understand all-payer’s potential is by recognizing the deficiencies with the current system. Premium prices are rising in the Obamacare exchanges. Insurance company UnitedHealth has openly discussed bolting from the exchanges, which would remove choices in some states and potentially increase premiums more. Finally, high deductibles make bronze-level insurance plans mostly unaffordable to actually use. Silver-level plans with higher premiums and cost -haring reductions make the coverage more viable, but takeup is uneven from state to state.
The cost of accessing coverage, or using it once you have it, has become a signature fear for consumers. There are two ways to deal with this: Increase subsidies so people can afford better insurance, or lower the overall cost of health care, which will subsequently lower the cost of premiums. How can we be sure that is true? Because there’s an Obamacare rule called the medical loss ratio that mandates insurance companies spend a set level of premium dollars on medical treatment, or else give their customers back a rebate. If you lower provider costs, insurers will have to pass that savings back to the public, by law.
That’s where all-payer rate setting comes in. This reform establishes either a government agency or a panel of private insurers that sets one distinct price for every medical procedure. Instead of different insurers bargaining with providers for a price for each service, it allows them to effectively band together and use their market power to get the best possible rate.
The current fragmented system—with different rates for Medicare, Medicaid, the Veterans Administration, and private insurance—allows providers to take advantage. This has driven much of the recent hospital consolidation, with health care providers merging to increase their bargaining power and raise prices. A backlash of insurance company consolidation has formed on the other side, but without an all-payer system that includes Medicare and Medicaid, banding together for bargaining leverage can only go so far.
Along with reducing the cost of health care, all-payer reduces insurers’ administrative costs, because instead of each company needing negotiators and billing clerks for each hospital chain, the prices are all deliberately laid out. It would eliminate the incentive for consolidation, and it actually might get insurers to compete for customers on things other than cost, like quality of service or perks to promote wellness. And because of the medical loss ratio, consumers would see their premium dollars stretch further for better coverage.
This vision of government-enabled price-fixing, while active in places like Germany and Switzerland, may sound fanciful for the United States. But many states have used all-payer systems at one time or another. Though successful at controlling costs, the programs withered during the Reagan era, which venerated market competition and dismissed interventions like rate-setting as failures that stifled innovation. Regardless of the truth, that label stuck.
Today we’re down to a limited version in West Virginia, and a more comprehensive system in Maryland, which includes Medicare rates. An independent state agency has set health care prices in Maryland since 1976.
During O’Malley’s tenure, Maryland instituted a complementary reform to all-payer. State hospitals had reacted to price controls over time by increasing the admission rate, maximizing profits through volume. So in 2014, Maryland revamped the system by setting a global budget for hospitals, delivering a fixed amount of money every year, adjusted for local demographics. This five-year demonstration project is in its experimental stages, but every hospital in the state signed up for the voluntary program within six months, and it has already saved more than $100 million for Medicare in the first year, with hospital readmission rates below the national average, according to data recently published in the New England Journal of Medicine.
The combination of all-payer and global budgeting reduces the incentive for constant hospital readmissions to maximize profits, and it allows hospitals to focus on prevention and prudent use of treatment to meet their defined budgets. This lets a successful hospital co-exist with a healthier community.
O’Malley’s health care plan, released yesterday, would encourage states to adopt global budgeting. But that tantalizing moment in the Democratic debate prevented O’Malley from bringing these ideas to the national stage. Instead of wrestling with the virtues of all-payer, we have only whistling-past-the-graveyard pronouncements that everything is fine with Obamacare, or demands to nationalize a major sector of the economy. Hillary Clinton’s plans to enhance Obamacare, mostly with tax credits for families with high health-care costs, have become bogged down in a philosophical argument with Bernie Sanders, with the Clinton camp vowing never to raise taxes on people making less than $250,000. Not only does such a pledge limit the promise of progressive politics, it unnecessarily shifts the health care debate into a tax debate.
All-payer offers a way out of this box. It also includes the one feature that appears necessary for passing legislation in the 21st century: industry support. Insurance companies like the certainty of all-payer and the increased bargaining power. And Maryland hospitals quickly signed up for the global budgeting project, perhaps for similar reasons as the insurers: the prospect of reducing administrative overhead, and focusing their work on innovation.
Single-payer remains part of the discussion on the left; in Colorado, it will be on the ballot next year. But all-payer achieves many of the goals of a single-payer system, and should get into this conversation as well. If it weren’t for John Dickerson and the tyranny of the CBS sponsors, it would have a couple of weeks ago.'
https://newrepublic.com/article/124584/best-health-care-fix-never-heard
 = new reply since forum marked as read
Highlight:
NoneDon't highlight anything
5 newestHighlight 5 most recent replies
= new reply since forum marked as read
Highlight:
NoneDon't highlight anything
5 newestHighlight 5 most recent replies
Samantha
(9,314 posts)I will try to come back later to finish reading it.
O'Malley is a great candidate, and it is disturbing the lack of exposure he has received in this contest.
Have a wonderful Thanksgiving.
Sam

elleng
(141,926 posts)and Happy Thanksgiving to you.


daybranch
(1,309 posts)It is fine to talk about all payer systems amnd many of the features can be successfully implemented in either the ACA or in Medicare for All. As it is most Americans are favoring a Medicare for all system and are dissatisfied with the lack of a public option or want Medicare for All. The mood of the country is not to support and enrich a do nothing medical insurance or pharmaceutical industry, especially as some try to avoid taxes by offshoring profits and combining with foreign firms. So yes, Mr. O Malley has a good half measure and maybe Hillary will adopt it as the queen of half measures , protecting her donor class. At this point it is unlikely in my humble opinion few Americans except centrists of which there are few would be interested in such half steps. maybe Hillary or President Obama would like the ideas, they seem to avoid real change.

Andy823
(11,555 posts)This five-year demonstration project is in its experimental stages, but every hospital in the state signed up for the voluntary program within six months, and it has already saved more than $100 million for Medicare in the first year, with hospital readmission rates below the national average, according to data recently published in the New England Journal of Medicine.
Lowering the cost of health care really needs to be done, and O'Malley is right.

kristopher
(29,798 posts)All you've done is divert away from the question, which is, what is the role of the insurance companies and why do we need them under this plan?
They are in place largely as a way to control health care costs. They aren't doing that and we need government intervention to accomplish that function. What value are the insurance companies bring to the table?
Also, how does the "all payer' approach help with the supply side of the equation? A large part of the structural problem lies in the extremely high costs incurred to put a health care provider on the front line. Those high costs are largely a function of the medical cartels controlling the supply. Without gaining control over the supply side, the cost saving system won't work. It will result (IMO) in a trend to redefine upwards the qualifications needed to deliver even the most rudimentary functions of health care - leading to health care provider shortages and cost increases that the all payer model can't control.
We already have a functioning template that can be easily expanded - Medicare. It does what we need to accomplish. Why make it more complicated? Why not try to turn out the voters we need to make REAL change happen?
hill2016
(1,772 posts)partially by people paying in for many years before they can use it?
riderinthestorm
(23,272 posts)Armstead
(47,803 posts)We either need to force the industry into a subservient role as hired functionaries.
hill2016
(1,772 posts)is thinking of pulling out of the exchanges?
if you don't make it worth their while (profits) they won't participate.
Armstead
(47,803 posts)It's not worth their while unless they gouge consumers to add profit to the mix.
That is the nature of health insurance. It is not a profitable business model, because it is dealing with totally uncontrollable factors of health and/or accidents, as well as widely fluctuating costs of providing healthcare.
That is why the system we have is not sustainable. If there are to be private insurance companies, they should be relegated to a role of contractor to the government for servicing public health plans.
Sorry if that sounds "socialistic" but many capitalist countries have a public health system (even when they are hybrids) and we should be moving in that direction too, rather than placating and propping up a system that is inherently a bad business model.

Enthusiast
(50,983 posts)GoneFishin
(5,217 posts)people again through out-of-pocket and deductible costs. Which is disgusting because most of us watching the ACA discussions watched the corporatists sucking up to the Health Insurance and Pharmaceutical industry and were angry as hell because this was very predictable.
hill2016
(1,772 posts)because the aca market is not profitable for them. which is why united health is thinking of pulling out.
the reason it is not profitable is because the young and healthy have not been buying in as much as is needed to support the older and sicker cohort who have been using more medical care than espected.

MFrohike
(1,980 posts)Nothing screams free market like guaranteeing profits in a captive market.
Sheesh.
Andy823
(11,555 posts)It really ticks me off when things like this don't make it into the debates, but bickering and arguing is always allowed.

eridani
(51,907 posts)single payer only refers to the payment of health services. it doesn't neccessitate cost control. conversely private insurers and pbms can also negotiate prices
eridani
(51,907 posts)--is in included.
Enthusiast
(50,983 posts)Dead weight like the insurance industry do not need to be included in health care reform. They are entirely parasitic in nature and do nothing but collect free money while they unnecessarily complicate every aspect health care delivery.
Andy823
(11,555 posts)This is an issue we should all be discussing instead of making stupid attacks at the "other" candidates. O'Malley has a real plan to fix things, yet people only seem to want fight and argue instead of talking about how to fix things.

Matariki
(18,775 posts)There is no good reason for Insurance companies to be profiting from health care. They have absolutely nothing to do with healing.
Aerows
(39,961 posts)Martin O'Malley has some extremely well-thought and proven ideas. I do NOT understand why more people are not on the Martin O'Malley bus.
It is stunning to me. Why is the media orchestrating a campaign to silence damn good ideas, and a damn good candidate like this?

Bread and Circus
(9,454 posts)hill2016
(1,772 posts)is how to deal with regional differences in costs?
otherwise it seems a surprisingly balanced article
Crystalite
(164 posts)Just reading that raised my blood pressure, reminded of the very obvious preferential treatment afforded the frontrunner throughout that debate.
I'd like to see the full set of rules and agreements that were in place.
Thank you for posting this, elleng, and Best Thanksgiving Wished to You and Yours!
elleng
(141,926 posts)Bread and Circus
(9,454 posts)I know hospitals do consolidate and are buying up doctors as a way to circle the wagons. However, independent physicians are legally prohibited from banding together to negotiate or set prices in a cartel like manner.
I can't complain as I make a lot of money but if health plans can form alliances to price set would physicians be allowed to do the same? Right now I can only negotiate my contracts as one person and there isn't really a negotiation. The contracts are take it or leave it.
Honestly though one price for me would be cool as long as medicaid was on the hook for that price. Many states peg medicaid reimbursement so low it is not feasible to render care unless your practice is subsidized.

Live and Learn
(12,769 posts)solutions such as this together. Perhaps we could actually come up with a great solutions.

Todays_Illusion
(1,209 posts)to eliminate Medicare and VA without an alternative other than more government meddling and tweaking.
A much easier way to reduce costs, and provide better care for more for less out of pocket and less would be to begin by lowering the Medicare age to 55.
Andy823
(11,555 posts)Andy823
(11,555 posts)

Jarqui
(10,924 posts)Last edited Sat Nov 28, 2015, 09:12 AM - Edit history (1)
They trot off with 20-25% of the healthcare dollars - maybe to an offshore tax free situation.
Insurance companies are in a conflict of interest "5% of patients won't live as long with this cheaper treatment but our bottom line will be 10% better!"
America can save roughly 20% of their healthcare dollars by getting the middleman (insurance companies) out of the way without compromising their quality of healthcare.
Some might say" that's un-American! - Commie-like" I might respond that profiting off the health misfortune of Americans and ignoring those who cannot afford it, leaving them to die (as 0.1% do - 33,000 per year) is even more un-American.
Health insurance costs have reached silly levels in the US. Nearly double most countries per capita spending while way down the list on life expectancy (34?). The high cost of health insurance doesn't just limit who can get it - it also hurts employment because other countries can provide cheaper labor just on the basis of the thousands extra in health care costs. Not being competitive is arguably un-American too.
To become competitive and affordable, every aspect of controlling healthcare costs should be on the table to reduce ridiculously high costs - beyond just removing the middle man insurance companies.
To me, the only answer that can do all of the above is single payer. For the good of the country and everybody in it except insurance company executives and shareholders, it's the way to go. Let's not waste any more time with bandaids that will not result in completely healing the healthcare wound.
Enthusiast
(50,983 posts)
Recursion
(56,582 posts)Last edited Sat Nov 28, 2015, 10:05 PM - Edit history (1)
The difference between the premiums private insurance takes in and the payments they give to providers is 4% of our national healthcare spending. It's irritating but not the problem; the 60% that physicians and hospitals take is the problem.
hill2016
(1,772 posts)in a single payer system. this shows up as spending on the services side.
it won't disappear entirely because you still need people to handle elective procedures or supplemental insurance.
Jarqui
(10,924 posts)I'm focused on private insurance which is about $1 trillion per year. If you chop 15% off that figure, it's $150 billion per year.
https://www.ehealthinsurance.com/resource-center/affordable-care-act/health-insurance-rebate
One major, yet little known, requirement of the Affordable Care Act (health care reform) was that a major medical health insurance plan be required to spend at least 80-85% of collected premium dollars on member medical care, beginning in 2011. This is the law’s so-called “medical loss ratio” rule.
Now, every year, insurers who don’t meet this medical loss ratio (MLR) requirement have to refund the difference to policyholders. Rebates are due no later than August 1.
and they have paid out:
Health Insurers Set To Give Out More Obamacare Refunds
http://www.huffingtonpost.com/2014/07/24/health-insurance-rebates_n_5614570.html
UnitedHealth
http://www.wsj.com/articles/unitedhealth-results-top-expectations-on-revenue-growth-1421839458
UnitedHealth said its medical-care ratio, a key industry metric that reflects the portion of insurance premiums used for patient care, fell to 79.8% in the fourth quarter from 81.2% a year earlier and was virtually flat from the 79.7% in the third quarter.
Anthem’s Medical Care Ratio Improves, Boosts Profit Margin
http://marketrealist.com/2015/04/anthems-medical-care-ratio-improves-boosts-profit-margin/
Anthem medical care ratio was 83.1% in 2014
Aetna medical-care ratio 83%
http://marketrealist.com/2015/03/star-ratings-increased-aetnas-government-sponsored-business-4q14/
So I'm not buying your 4% figure. These blood suckers are in this game to make serious money.
Now from that money, the insurers have to pay management mega-millions, salesmen, adjusters who screw consumers, billing staff and collectors, many lawyers, etc. A bunch of those dollars disappear with single payer because those functions are either not needed or needed substantially less or for a substantially more reasonable rate. Federal single payer becomes closer to a health provider verification and payment service who haggle deals to get better prices - no profit, much less administration and overhead. The consumer saves BIG on that.
Health insurance paperwork wastes $375 billion
http://www.cnbc.com/2015/01/13/health-insurance-paperwork-wastes-375-billion.html
The United States health-care system wastes an estimated $375 billion annually in billing and insurance-related paperwork that could be saved if the nation moved from a "multipayer" health coverage system to a "single-payer" system run by the government, a new study says.
That $375 billion doesn't cure a soul or do anything to improve medical outcomes. It's pure fat that costs each and every single American alive today about $1,179 per year or an American family of four $4,717 per year. It's stupid money down the inefficiency toilet that doesn't do nearly any one any good. It needs to go.
you were focused on the private insurance.
the article you cite and the figure of 375b includes government programs and is 15% of total health care spend.
Jarqui
(10,924 posts)" Private insurers contributed the largest share of BIR (Billing and insurance-related administrative) costs, $198 billion; public insurers contributed $35 billion."
You have to use your head a little. The public insurers are closer to single payer in spirit and structure.
I don't care which study or what nitpicking you want to go with. We're not doing an audit here. We're talking policy. I used different sources saying slightly different things to substantiate the overall general message. Private insurers are still making a bundle and costing Americans hundreds of billions needlessly. Single payer is the only path that is going to get US healthcare costs competitive with the rest of the world and solves this problem once and for all by saving Americans hundreds of billions in healthcare costs annually.
Recursion
(56,582 posts)Go here:
https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/NationalHealthExpendData/NationalHealthAccountsHistorical.html
And download these spreadshhets:
https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/NationalHealthExpendData/Downloads/Tables.zip
In 2013, private insurance took in $961B in premiums and paid out $846B to providers, for $115B in overhead, or 4% (actually about 3.8%) of the $3T the US spent on healthcare.
In the same year, Medicare and Medicaid took in $1T in levies and trust fund money and paid out $926B to providers, for $74T in overhead, or 2% of the $3T the US spent on healthcare.
CMS is literally just counting money that goes in and out; there's really no way around this.
That 4% is irritating, but just not the problem. "The" problem (to the extent that there is "one" problem) is that hospitals and doctors here make much, much more than hospitals and doctors in other countries do. Without direct provider reform we're going to keep paying much more than the rest of the world.
Jarqui
(10,924 posts)115B or 961B is 12.0 % of those private insurance dollars (without me looking up whether I agree with these figures). And a bunch of that $115 billion can be gotten rid of with single payer - more than all-payer or the ACA.
Further, when you go down through the hospitals and doctors, with single payer, further administration costs disappear at a roughly similar rate because for the most part, they're dealing with the Federal single payer system. They're not dealing nearly as extensively with patients, as many insurance companies as frequently, collection agencies, red tape, etc on administration.
As well, the average US deductible (ballpark) is $1,135. In Canada's single payer, apples to apples, there is no deductible. The above math focused on premiums and payout seems to overlook that but comes out of American's wallets. Studies looking at premiums and payout to providers either ignores the deductible or lowers the medical ratio.
Canada covers ALL of it's citizens with no deductible for 62.5% of the US health costs per capita and Canadians have a longer life expectancy. It's a rough example of what is possible in the US with single payer.
http://data.worldbank.org/indicator/SH.XPD.PCAP
Using Canadian single payer rates as a target, the US savings for single payer might roughly be:
US healthcare costs per capita..... $9,146
- CDN healthcare costs per capita - $5,718
============================
US Single payer savings per capita $3, 460
$3,460 savings per capita x 318 million US population = $1.1 Trillion per year
Or we could say the savings from spending 62.5% of the $3 trillion the US currently spends is $1.1 Trillion.
So that's a fair cross check to reinforce that talking about hundreds of billions of dollars in savings for the US to migrate to a single payer system like Canada has is not beyond the realm. That's the order of magnitude. Not the tiny 4% you claim - it's closer to ten times that.
It's massively BIG BIG bucks.
Recursion
(56,582 posts)what a small percent that was. Now you're talking about the percent of private insurance spending, which, yes, is about 12%, as compared to the 6% overhead Medicare has and the 9% overhead Medicaid has. (CHIP, meanwhile, has 12% overhead, and workers' comp. has 25% overhead.)
It's massively BIG BIG bucks.
Well, again, no; not really. It's a very small fraction of what we spend on healthcare. About 4%, in fact. It's not the problem. We spend 18% of our GDP on health care as opposed to about 10% in most OECD countries. We can't fix that by cutting 4% of our healthcare spending. We can fix it by drastically lowering the 60% of our healthcare spending that goes to physicians and hospitals.
As well, the average US deductible (ballpark) is $1,135.
Note that that's roughly the deductible that people in Norway, Denmark, and Australia pay in their public health systems, and close to France's out of pocket maximum, which I think is around $1400 at this point (but in France you have a 30% copay for everything, rather than a straight-up deductible).
Canada does have a system that's absolutely free at delivery, which is awesome, but that's incredibly unusual in the developed world; really just Canada, the UK, and Austria. That's not to say it can't work here, but if the majority of the OECD doesn't do it that way there's probably a reason.
Jarqui
(10,924 posts)They're positions you've misunderstood, twisted, cherry picked or you're creating a straw-man.
I'm not talking about cutting 4% of healthcare spending. That's your bogus cherry picked number. Not mine.
You raised Norway, Denmark, Australia and France.
Norway's per capita spending is like the US so I don't think we want to mimic them.
http://data.worldbank.org/indicator/SH.XPD.PCAP
Denmark is spending $6,270 per capita. If the US did that, the US would save (ballpark) $943 billion per year on healthcare
Australia is spending $6,110 per capita via a universal system - like single payer with deductible. If the US did that, the US would save (ballpark) $996 billion per year on healthcare
France is spending $4,864 per capita via a universal system - like single payer with deductible. If the US did that, the US would save (ballpark) $1.3 Trillion per year on healthcare
You can pick quite a few countries and mimic what they do and save hundreds of billions of dollars
NY Times
http://www.nytimes.com/roomfordebate/2015/10/20/can-the-us-become-denmark/us-health-care-could-be-more-like-denmarks
Aetna keeps 19 cents of every premium dollar for overhead and profit, leaving only 81 cents for care. And U.S. hospitals devote 25.3 percent of total revenue to administration, reflecting the high cost of collecting patient copayments and deductibles, and fighting with insurers.
...
In contrast, insurance overhead in single-payer programs (and fee-for-service Medicare) takes only 1 percent to 2 percent. In these programs, hospitals don't need to bill each patient; they're paid a lump sum budget, the way we fund fire departments, sharply cutting hospital administrative costs. Moving to a single-payer system would save about $400 billion annually on paperwork and administration — enough to ensure every American top coverage.
There's that darn $400 billion savings claim again (13.3% of total healthcare spending - not 4%)!!
Recursion
(56,582 posts)If we had a board, like they do, and like O'Malley is proposing, that said "regardless of the financing, a leg MRI can only cost $500, period" then we would save money like they do.
It doesn't really matter how we finance it. Seriously.
If we regulate costs like Europe does, we will (wait for it...) have lower costs, like Europe does. It doesn't matter at that point if we have single payer like Canada or a private insurance mandate like the Netherlands or a multi-tier system like France.
They haven't found some magic financing silver bullet (as witnessed by the fact that they use such different financing models), they've just set legal limits to costs.
Jarqui
(10,924 posts)Again:
Health insurance paperwork wastes $375 billion
http://www.cnbc.com/2015/01/13/health-insurance-paperwork-wastes-375-billion.html
"The United States health-care system wastes an estimated $375 billion annually in billing and insurance-related paperwork that could be saved if the nation moved from a "multipayer" health coverage system to a "single-payer" system run by the government, a new study says."
and:
NY Times : "Moving to a single-payer system would save about $400 billion annually on paperwork and administration"
http://www.nytimes.com/roomfordebate/2015/10/20/can-the-us-become-denmark/us-health-care-could-be-more-like-denmarks
In the above two independent assessments, this claim of yours is not correct or accurate: "it doesn't matter at that point if we have single payer like Canada or a private insurance mandate" It does matter some.
First of all, a bunch if not all of those cost reductions they're talking about - both estimates around $400 billion - are from paperwork inefficiencies and admin - not from folks setting cost limits.
For example, when someone sees a doctor in Canada, about 2-3 human beings are involved: the doctor, receptionist (who handles the single payer transactions from swiping the health card) and sometimes a nurse. When someone sees a doctor in the US, about 7-8 people are involved. The same three as Canada plus insurance staff plus other doctor/hospital admin staff, bill collector, etc. Everything else is the same.
Private insurance for all can get you a significant way there. Single payer is the most efficient because the private insurance companies have to make a profit and they're a middle man - introducing inefficiencies - another body - into the transactions because you require oversight by the government. Those that opt for non-profit private insurance - that helps get them closer to single payer.
If single payer gets you $400 billion in annual savings, deviations from that get you many billions of dollars less - depending on how much administration fat/waste/inefficiency is left in your flavor of deviation from single payer.
So what is easier, having to haggle with a bunch of insurance company middle men in determining how to effectively operate an electronic medical records system and have intermediate transactions that take longer OR one single payer who works it out and manages it directly with the hospitals and doctors with one transaction?
http://www.ehealthontario.on.ca/en/ehrs
The insurance companies "we don't want our competitor to know our data ... blah, blah, blah ... We want this data format for Xrays or else we won't play!!" etc, etc Just one more example of how single payer is easier.
All systems, even the current ACA, have areas of cost reduction they can seek independent of the type of system: single payer, two-tier, etc. They can set legal limits to costs - regardless of the system. So we agree on that part. But for reasons that should be obvious, single payer is the most efficient.
hill2016
(1,772 posts)here's another point you should consider
private insurance funds roughly 30% of US health care spending. let's call it 900b in premiums collected out of 3 trillion.
out of this, roughly 100b goes to health insurance companies (processing, underwriting, fraud detection, litigation, marketing, and of course profits). most of this cost could be cut out by going to single payer, which would have its own administartive costs though.
on the providers front, how much could be saved by getting rid of all the administrative costs in dealing with many insurance companies vs a government agency? i'm thinking at least 10 - 20 %. of course this number is pulled out of my ass, but next time talk to your doctor how much he could save if he only had to deal with one government entity.
so if we look solely at the private insurance part, there could be substantial savings there in moving to single payer.
Recursion
(56,582 posts)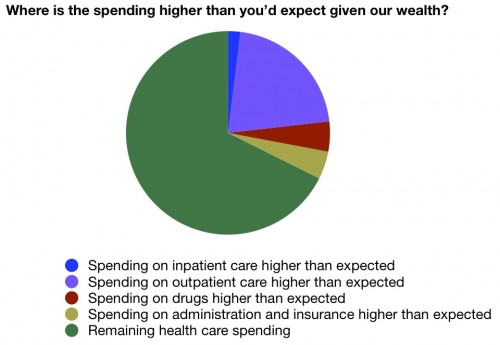
That small sort of beige wedge is the amount we pay above the OECD per capita baseline in all administrative costs, including providers' admin expenses, insurance administration and profit, and public financing administration.
Again, irritating, but not the dragon to slay. The problem is we pay absurdly more for outpatient care than anybody else in the world.
House of Roberts
(6,634 posts)That’s where all-payer rate setting comes in. This reform establishes either a government agency or a panel of private insurers that sets one distinct price for every medical procedure. Instead of different insurers bargaining with providers for a price for each service, it allows them to effectively band together and use their market power to get the best possible rate.
What a lot of people miss about the medical loss ratio rules of the ACA, is that when insurance companies negotiate provider prices DOWN, the accompanying profit available (15% for plans, 20% for individuals) DROPS also. The only way for the insurers to make more money now, is to pay MORE to providers, so the percentage they can charge on policies can go up.
O'Malley either doesn't know this, or he doesn't think people can figure this out.
Jarqui
(10,924 posts)trying to make major bucks on top of doctors and hospitals trying to make major bucks, you're going to have a cost containment problem.
Even if they get the insurers out of the way, they're still going to have problems with doctors and hospitals, etc wanting their bigger piece of the American dream.
But I think it's fair to say that in general, the insurers have compounded the problem because their take is a % on top of a %.
I've seen 4% as a figure for the single payer admin costs vs 15-20% insurance company margin now. Beyond that gross admin savings, there are further savings to be achieved below that (some are laid out in the ACA)

ms liberty
(11,364 posts)K&R
elleng
(141,926 posts)Happy Thanksgiving!
Cheese Sandwich
(9,086 posts)No aid and comfort for the enemy.
hill2016
(1,772 posts)the premiums on the individual market have to be signed off by state regulators? who check through their acturial costs very carefully?

Kick in to the DU tip jar?
This week we're running a special pop-up mini fund drive. From Monday through Friday we're going ad-free for all registered members, and we're asking you to kick in to the DU tip jar to support the site and keep us financially healthy.
As a bonus, making a contribution will allow you to leave kudos for another DU member, and at the end of the week we'll recognize the DUers who you think make this community great.