eridani
eridani's JournalInsurers Profit From Health Law They Fought
http://www.bloomberg.com/news/2012-01-05/health-insurer-profit-rises-as-obama-s-health-law-supplies-revenue-boost.htmlInsurance companies spent millions of dollars trying to defeat the U.S.health-care overhaul, saying it would raise costs and disrupt coverage. Instead, profit margins at the companies widened to levels not seen since before the recession, a Bloomberg Government study shows.
Insurers led by WellPoint Inc. (WLP), the biggest by membership, recorded their highest combined quarterly net income of the past decade after the law was signed in 2010, said Peter Gosselin, the study author and senior health-care analyst for Bloomberg Government. The Standard & Poor's 500 Managed Health-Care Index rose 36 percent in the period, four times more than the S&P 500.
"The industry that was the loudest, most persistent critic of this law, the industry whose analysts and executives predicted it would suffer immensely because of the law, has thrived," Gosselin said. "There is a shift to government work under way that is going to represent a fundamental change in their business model."
The Bloomberg Government report is available only to subscribers, but Peter Gosselin provides the essence of his conclusions in the brief video available at the link above. Peter Gosselin discusses his report, "Despite Predictions, Health Insurers Prosper Under Overhaul" (5 minute video):
Comment by Don McCanne of PNHP: Peter Gosselin's Bloomberg Government report, "Despite Predictions, Health Insurers Prosper Under Overhaul," is further confirmation that, as long as we leave the private insurers in charge, they will always find a way to stick it to us, as we now witness a dramatic increase in insurers cornering taxpayer-financed health insurance programs- Medicare and Medicaid - not to mention the private plans that taxpayers purchase for government employees on all levels.
These trends are very healthy for the private insurance industry, but they're enough to make us sick.
President Obama: Reject the Institute of Medicine's skimpy health plan prescription!!
A recent Quote of the Day message expressed alarm at the fact that the Institute of Medicine is recommending a grossly inadequate, skimpy, spartan standard for the package of benefits to be offered by health plans in the state insurance exchanges being established under the Affordable Care Act:
http://www.pnhp.org/news/2011/october/ioms-disturbing-report-on-essential-health-benefits
Following is a letter asking the Obama administration to reject this recommendation. Though only selected names will be used in publicizing this letter, we encourage everyone who concurs with the views expressed to sign it, using this link:
http://www.pnhp.org/iom-letter/index.php?UID=1348
We protest the Institute of Medicine’s (IOM) recommendation that cost rather than medical need be the basis for defining the “essential benefits” that insurance policies must cover when the federal health reform law takes effect in 2014. If adopted by the Department of Health and Human Services, this recommendation will sacrifice many lives and cause much suffering. We call on Secretary Sebelius and President Obama to reject them.
The IOM proposal would base the required coverage on the benefits typical of plans currently offered by small businesses – enshrining these skimpy plans as the new standard. These bare-bones policies come with a long list of uncovered services and saddle enrollees with unaffordable co-payments and deductibles.
Already, millions of underinsured Americans forgo essential care: adults with heart attacks delay seeking emergency care; children forgo needed primary and specialty care; patients fail to fill prescriptions for lifesaving medications; and serious illness often leads to financial catastrophe.
The inadequate coverage the IOM recommends would shift costs from corporate and government payers onto families already burdened by illness. Yet this strategy will not lower costs. Delaying care frequently creates even higher costs. Steadily rising co-payments and deductibles over the past two decades have failed to stem skyrocketing medical inflation. And nations that assure comprehensive coverage – with out-of-pocket costs a fraction of those in the United States – have experienced both slower cost growth and greater health gains than our country.
Our patients urgently need what people in these other nations already enjoy: universal and comprehensive coverage in a nonprofit system that prioritizes human need over corporate profit.
The IOM committee was riddled with conflicts of interest, many members having amassed personal wealth and career success through their involvement with health insurers and other for-profit health care firms. Its recommendations were lauded by insurance industry leaders who have sought to undermine real health reform at every turn. As the Lancet noted on its Dec. 5, 2009, cover: “Corporate influence renders the U.S. government incapable of making policy on the basis of evidence and the public interest.”
Sadly, the committee’s damaging recommendations suggest that this corporate bug has also infected the IOM.
Political problems with private insurance mandates
The author's question about Medicare is pretty easy to answer. It is financed by a tax, and the benefits are the same for everyone. You have surely all noted the massive unpopularity of Medicare privatization via vouchers. ACA is essentially a voucherized "Medicare" for people under 65, who don't like it any better than the over 65 crowd does.
http://www.tnr.com/print/article/politics/99072/the-health-care-mandate-really-was-mistake
I understand the impulse to defend the Affordable Care Act when it is under unrelenting attack. But a mistake is a mistake, and supporters of the law—particularly Democratic candidates facing tough races in 2012—need to think through alternatives to the mandate in view of both the upcoming Supreme Court ruling and this fall’s election.
Whether the Court will overturn the mandate, we don’t know. But in drafting the Affordable Care Act, Democrats put at unnecessary risk their most significant domestic achievement of the past three years. Keeping the same policy, they could have framed the mandate so it fell unambiguously under the government’s taxing power. Even just labeling the penalties for failing to insure a “tax” would have strengthened the argument for upholding the law and greatly increased the odds that the Court would invoke the 1867 Anti-Injunction Act, deferring the case until 2015, when the penalties would first be imposed. And Democrats could have avoided any constitutional challenge by adopting the alternative that I proposed, which eliminated the mandate by providing for a long-term (five-year) opt out from both the law’s benefits and its penalties.
That the mandate was a political as well as a legal miscalculation should also now be clear. When Congress passed the Affordable Care Act, many observers expected that controversy would die down, and the law would soon be as widely accepted as Medicare is. That hasn’t happened. Why not?
The mandate is one reason why the law’s opponents have been able to sustain their cause. No other provision could have provided as effective a basis for both the legal challenges to the law and the political campaigns against it; voters in 14 states have passed amendments to their state constitutions prohibiting an individual mandate. Even though such amendments have no legal force, the campaigns and court cases have kept public opinion focused on the least popular aspect of the Affordable Care Act, dragging down overall support and maintaining the high-intensity opposition to the law on the right (in contrast to the tepid and ambivalent support for it on the left).
In Dire Health
In Dire Health
By Arnold S. Relman
Most people assume that insurance is an essential part of the health-care system. Some think it should be provided through public programs like Medicare, while others prefer to see it purchased from private insurance companies, but the majority believe that insurance is needed to help pay the unpredictable and often catastrophic expenses of medical care. That is why so much public policy focuses on extending coverage to as many people as possible and controlling its cost. I think this emphasis on insurance is mistaken. We would have a much better and more affordable health-care system if the reimbursement of medical expenses through public or private insurance plans was replaced by a tax-supported universal access to comprehensive care, without bills for specific services and without insurance plans to pay those bills.
<snip>
For-profit insurance companies, which control most of the private market, are the greatest problem. They have a direct conflict of interest with their customers, because a plan's net income is increased by avoiding coverage of patients with serious illness (who, of course, are most in need of insurance), restricting access to services, and limiting coverage of expensive medical services.
There is, however, a practical alternative to health insurance and the fee-for-service system with which it is usually associated: a not-for-profit system in which a public single payer provides universal access to comprehensive private care delivered by primary-care physicians cooperating with medical specialists in group-practice arrangements.
I do not underestimate the complexity of the changes I am proposing. The odds against it are daunting. Congress might not even begin to debate major reform until the health system is near collapse. But what seems clear is that the best - possibly the only - hope for achieving universal, affordable care lies in the eventual elimination of private insurance and fee-for-service payment and in the creation of a tax-supported system based on group practice. Although this proposal makes good medical, social, and economic sense, its ultimate fate will be decided in the political arena. It cannot become a reality without an informed and aroused public bolstered by the medical profession's strong support for the reform.
(Arnold S. Relman is a professor emeritus of medicine and social medicine at Harvard Medical School and the former editor of The New England Journal of Medicine.)
Comment by Don McCanne of PNUP: It seems appropriate to begin the new year with the words of the venerable Arnold Relman. Much media attention on reform will be misdirected this year to implementation of the private-insurance-based Affordable Care Act and to its challenge in the U.S. Supreme Court. Dr. Relman reminds us that instead we need to move forward with informing and arousing the public in support of fundamental reform that actually would bring affordable care to all.
If you were a taxonomist, you would have to classify Dems and Repubs as different species
Conservation voters ratings of the 2008 WA State legislature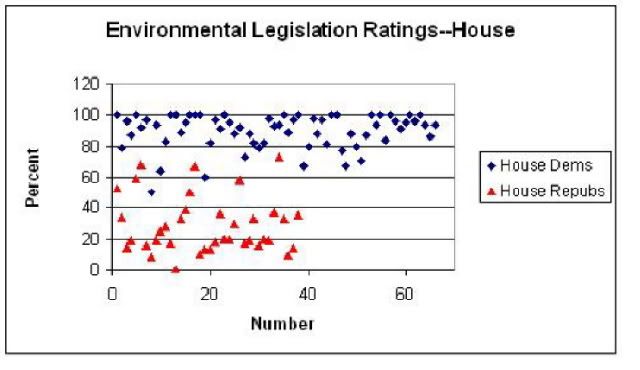
Alliance of Retired Americans rating of 2005 Congress on senior issues
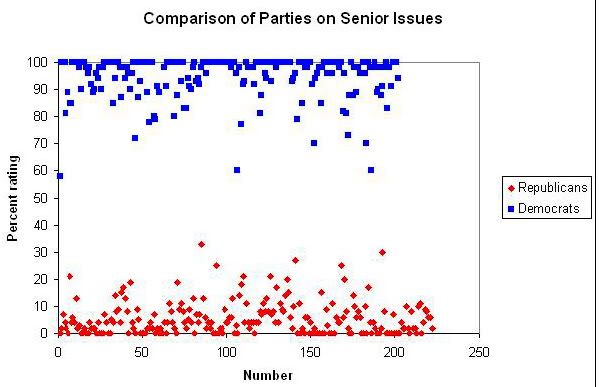
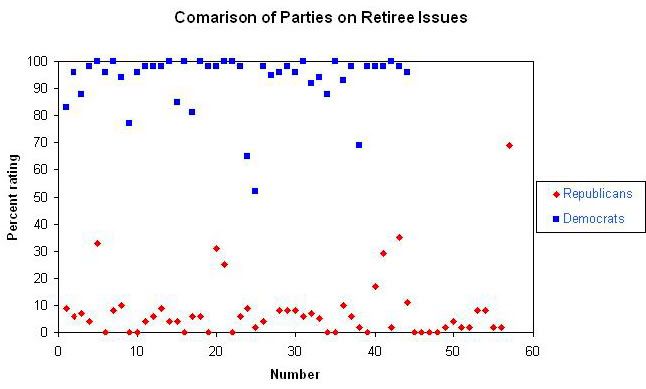
Votes are ranked on a scale of 0 to 100, with Republicans clustering around 0, and Democrats clustering around 100. So the reason why unions, feminists, environmentalists, etc. stick with Democrats is that Democrats overwhelmingly vote the right way on their issues and Republicans almost never do.
From a progressive standpoint, of course, the obvious problem is that the bold, transformative stuff like single payer or EFCA never makes it out of committee. And that is never going to happen unless OWS and similar groups become permanent outside pressure groups. It would be helpful if progressives would get better at doing electoral politics, so that we could primary more Democrats who need it. All too many progressive issue junkies refuse to recognize that most voters don't happen to be committed policy wonks.
BTW, the most conservative Democrats have better voting records than the most liberal Republicans. For all 222 House Republicans in 2005, the average score was 5.5 (standard deviation 6.2). For the 203 Democrats, the average score was 94.6 (standard deviation 8.0). Rating a Democrat as conservative with a score of less than 85, there are only 19 of them--with average score of 75.8 (standard deviation 8.8). Rating a Republican as liberal with a score of more than 15, there are only 16 of them--with average score of 22.2 (standard deviation 4.6).
High-deductible health plans on the rise
Corporate employers, small businesses and nonprofit organizations are increasingly requiring their workers to spend between $1,200 and $5,000 before filing a health insurance claim.
Nearly three in four employers will offer at least one of these plans next year, according to a survey by the National Business Group on Health, a nonprofit association that represents large employers.
Helen Darling, its president, predicts that by 2016 the majority of all health plans will have high deductibles.
Comment by Don McCanne of PNHP: The National Business Group on Health (NBGH) is composed of the nation's largest employers, predominantly Fortune 500 companies. They provide health coverage for over 50 million workers, retirees and their families. When NBGH's president, Helen Darling, says that three years from now the majority of all plans will have high deductibles, you can bank on it.
Although this development is independent of the measures in the Affordable Care Act (ACA), it has greater consequences than any other feature of ACA, merely based on the number of people who will be impacted - not just the Fortune 500 company employees, but virtually everyone else as well.
Most workers and their families obtain their health care coverage through their employment. With large employers leading the way, high deductible plans will become the national standard. For median-income households, the deductible is large enough to create a financial hardship should a family member have significant health care needs. Thus, under-insurance is becoming the new norm, not only for employer-sponsored plans, but also for the low actuarial value plans to be offered through the state insurance exchanges.
The rationale usually given for high deductibles is to make patients more sensitive to the costs of health care so that they will use less of it. This has been shown not only to decrease the use of beneficial health care services, but it also potentially exposes people to financial hardship when they develop problems for which health care is absolutely essential.
So the question is, does this really save enough money to warrant these adverse consequences? Let's look at the RAND HIE and also the experiences of other nations.
The RAND Health Insurance Experiment demonstrated that health care use was reduced by 30 percent in patients with cost sharing as compared to first dollar coverage, supposedly without resulting in harm (though low-income people were harmed). But that study was limited to healthy workers and their young healthy families during a few healthy years of their lives. It does not apply to the relatively unhealthy 20 percent of people who use 80 percent of our health care dollars - care that is not influenced by deductibles. Reducing spending by 30 percent on healthy people who use very little care - perhaps an office visit or two - is not going to reduce our national health expenditures significantly.
Many other nations have first dollar coverage with no deductibles, yet spend far less than we do, and with no evidence of significant overuse of medical services. There are far more effective and much more patient-friendly methods of controlling spending than the use of deductibles and other cost sharing, as these nations have demonstrated.
The Affordable Care Act is not providing us the framework that would ensure affordable care for everyone. Trying to modify the Act to make it work better won't help because the financing infrastructure is so fundamentally flawed that legislative tweaking cannot repair it. Though getting rid of deductibles would be an improvement, it wouldn't reduce our high costs, but would merely shift them, making insurance premiums even less affordable.
For this new year, we really have our work cut out for us. The public at large needs to understand the irreparable flaws in the ACA model of reform. People need to know that we can control spending while making health care accessible and affordable for everyone. We can do this by enacting a far better way to finance health care - a single payer national health program: an improved Medicare for all.
My comment: Not only do the sickest 20% account for 80% of health care costs, 5% of the very sickest account for 50% of the costs. "More skin in the game" really means "Save money by bankrupting and killing the very sickest."
The Ones Who Walk Away from Omelas
The Ones Who Walk Away from Omelas (Variations on a theme by William James) is a short story by Ursula K. Le Guin. It won the Hugo Award (in science fiction) for short stories in 1974.In the story, Omelas is a utopian city of happiness and delight, whose inhabitants are smart and cultured. Everything about Omelas is pleasing, except for the secret of the city: the good fortune of Omelas requires that a single unfortunate child be kept in perpetual filth, darkness and misery, and that all her citizens should be told of this on coming of age.
After being exposed to the truth, most of the people of Omelas are initially shocked and disgusted, but are ultimately able to come to terms with the fact and resolve to live their lives in such a manner as to make the suffering of the unfortunate child worth it. However, some few of the citizens, young or old, silently walk away from the city, and no one knows where they go. The story ends with "The place they go towards is a place even less imaginable to us than the city of happiness. I cannot describe it at all. It is possible it does not exist. But they seem to know where they are going, the ones who walk away from Omelas."
You can read the story in its entirety at http://harelbarzilai.org/words/omelas.txt or www.markaelrod.net/wp-content/uploads/2006/05/omelas.pdf The following is a brief excerpt—
In a basement under one of the beautiful public buildings of Omelas, or perhaps in the cellar of one of its spacious private homes, there is a room. It has one locked door, and no window. A little light seeps in dustily between cracks in the boards, secondhand from a cobwebbed window somewhere across the cellar. In one corner of the little room a couple of mops, with stiff, clotted, foul-smelling heads, stand near a rusty bucket. The floor is dirt, a little damp to the touch, as cellar dirt usually is.
The room is about three paces long and two wide: a mere broom closet or disused tool room. In the room, a child is sitting. It could be a boy or a girl. It looks about six, but actually is nearly ten. It is feeble-minded. Perhaps it was born defective, or perhaps it has become imbecile through fear, malnutrition, and neglect.
They all know it is there, all the people of Omelas. Some of them have come to see it, others are content merely to know it is there. They all know that it has to be there. Some of them understand why, and some do not, but they all understand that their happiness, the beauty of their city, the tenderness of their friendships, the health of their children, the wisdom of their scholars, the skill of their makers, even the abundance of their harvest and the kindly weathers of their skies, depend wholly on this child's abominable misery.
Le Guin’s commentary—
http://en.wikipedia.org/wiki/The_Ones_Who_Walk_Away_from_Omelas
"The central idea of this psychomyth, the scapegoat", writes Le Guin, "turns up in Dostoyevsky's Brothers Karamazov, and several people have asked me, rather suspiciously, why I gave the credit to William James. The fact is, I haven't been able to re-read Dostoyevsky, much as I loved him, since I was twenty-five, and I'd simply forgotten he used the idea. But when I met it in James's The Moral Philosopher and the Moral Life, it was with a shock of recognition."
The quote from William James is:
Or if the hypothesis were offered us of a world in which Messrs. Fourier's and Bellamy's and Morris's utopias should all be outdone, and millions kept permanently happy on the one simple condition that a certain lost soul on the far-off edge of things should lead a life of lonely torture, what except a specific and independent sort of emotion can it be which would make us immediately feel, even though an impulse arose within us to clutch at the happiness so offered, how hideous a thing would be its enjoyment when deliberately accepted as the fruit of such a bargain?
Le Guin hit upon the name of the town on seeing a road sign for Salem, Oregon, in a car mirror. “[… People ask me] ‘Where do you get your ideas from, Ms. Le Guin?’ From forgetting Dostoyevsky and reading road signs backwards, naturally. Where else?”
We all are living in Omelas right now
I’m sure that, given all the on-line debates over the 2010 health care bill, it’s pretty obvious where I’m going with this. According to the best of our American values, what we should have gotten was what citizens in every other part of the developed world take for granted—access to health care for all citizens, no exceptions. Apparently the best we can manage is eventual access to inadequate insurance for most of us, and what we got reflects our very worst values, chief of which is that your access to health care should depend mostly on how much money you have. Our brave new call to solidarity is “An injury to one is, after all, only an injury to one. Just ignore it and count your blessings.”
Yes, with more subsidized access to insurance, even inadequate insurance, fewer will die. Given that in nine years 35 million will still lack such access, instead of 46,000 dying a year, there will be 15,000 or fewer dying nine years from now. Kids with pre-existing conditions will no longer be denied coverage as of right now, but their parents will have to wait until 2014. Young adults 23-26 can remain on their parents’ plan, except for those whose parents don’t have insurance, can’t afford to add them, or kicked them out of the house years ago.
We have indeed made a start on emptying out our room full of non-persons, though we are nowhere near getting the number down to one as the fictional citizens of Omelas did. You see the big problem with the slowly emptying room, I hope. The lower the number of people still in it, the easier it will be for everybody else to ignore them permanently.
That has been our biggest political problem in trying to achieve universal health care all along—about 85% of us are never going to get really expensively sick. 5% of the population in every age group accounts for 50% of the health care expenses for that group. 15% account for 85%, and line of least resistance for the remaining mostly healthy 85% is to just ignore the unfortunates hidden in the basement. The healthy majority remains free to think that such insurance as they have is probably pretty good, an opinion about as well-informed as their opinions about how good their fire extinguishers are. After all, 46,000 dead is less than a tenth of a percent of the population; 350,000 bankruptcies amounts to only 1% of the population. According to the California Nurses study, 21% of claims are denied, which means that four out of five are not denied. If most people are just fine, it’s very easy for them to ignore the small minority who are not.
No, I am not happy at all about “reform,” and even the batshit crazy sociopathology of its right wing opponents doesn’t change that for me. Le Guin’s fictional solution of just leaving Omelas won’t work for me either, though it has for people like one of the former chairs of Health Care for All-WA. Dr. Bramhall used to be the only MD psychiatrist in Washington State who would see Medicaid patients. Her reimbursments had dwindled for years. She gave up her car and moved to an apartment on Pill Hill near her practice to save money and keep helping the desperate people she worked with. Eventually, she could not afford health care for herself, a very bad situation for someone of late middle age to be in. Luckily for her, New Zealand was very happy to pay for her health care in exchange for making her professional skills available to their population.
Permanently breaking down the door to the basement room is the only thing that will get everybody out of our Room of Non-Persons Who Don't Deserve Health Care. I truly believe that most of the people cheering in the streets for the release of some fully intend to go back down at some time or another for the rest. But, based on quite a bit of past history, if that were really likely to happen Le Guin would never have felt the need to write her story at all.
Why the Wyden-Ryan plan amounts to privatization of Medicare
http://www.commondreams.org/view/2011/12/25-0?printWhy does the Wyden-Ryan plan amount to privatization? A brief glance at the recent history of Medicare is necessary to explain.
Medicare was once dominated by the federal government, where, as a result, administrative costs were low and quality was high. In the 1990's Medicare patients were given an option to have their Medicare services performed by private providers, who were now able to profit off Medicare by charging extra fees for extra services, which they added to the basic amount of funds received via Medicare.
The reason that people often chose private providers was that Medicare funding was being cut and consequently, less services were being offered under traditional Medicare. For those who could afford it, private providers became preferred, since people could then purchase the services they needed but were not offered under traditional Medicare. This "option" created the beginning of a two-tier system of Medicare, opening the door for the systems fracturing.
The Wyden-Ryan plan would crack the nut wide open. But instead of saying privatization, a dirty word, "premium support" is used instead, a sterile sounding term with nasty consequences. It essentially means that each Medicare patient will receive a set amount of money for their Medicare that they can use to "shop" for their insurance. This would be the first time that Medicare spending would be capped, and the rate of growth of this capped fund would not match the rate of growth of health care prices. Once you've accepted the cap, the cap can be continually lowered by Congress or not raised to keep pace with inflation.
Instead of reducing Medicare costs by going after profit-hungry pharmaceutical corporations, patients will have their services curtailed via the cap
+10000!! n/t
What I really expected from Obama--
--was that he would run his administration like he ran his campaign. When it came down to Obama or Clinton, it made no difference to me one way or the other on the issues. Both are confirmed corporatists. Obama was slightly better on the wars, and Clinton slightly better on health care. Both were mostly funded by the same corporate interests.
I made my choice to support Obama strictly on the grounds of his campaign organization. In our caucus state, the Clinton people came in and told local Dems that they'd better get behind the inevitable winner, or those wanting political careers would be made to pay. And she hired worthless pieces of shit like Mark Penn.
Obama, on the other hand, hired experienced organizers and used a lot of his early financial booty to set up software that people could use for self-organization. The paid people came in and mostly approved of what local people were already doing. They contacted local party leaders and PCOs, and listened to what we had to say.
The 2008 general election was THE canonical model for how elections should always be run. In past years, the "coordinated" campaign, supposedly working on state and national candidates concurrently, has always been totally uncoordinated chaos, featuring newbies who blew into town and did their own thing, totally ignoring what local party members were already doing. I don't know how many times I answered calls for door-knocking volunteers and wound up walking a precinct that already had literature hanging from all the doorknobs, put there by a local PCO.
In 2008, the people sent from the national organization immediately connected with the local party people. They asked us for lists of precincts with and without PCOs, and accepted our evaluation of just how likely any given PCO was to actually walk his or her precinct. My legislative district contains parts of 3 congressional districts and 5 cities, so I recommended subdivisions by geography which the coordinators immediately accepted. With a near-perfect blend of the online campaigning pioneered by Dean and tradtional personal outreach, there was this very rewarding sense of being on the same page as everyone else and getting something done right for a change.
Silly me. I expected that to carry over into Obama's administration. When OFA became Organizing for America, all that changed. No one wanted to hear what any of us local people had to say anymore. We were given the word from on high about priorities, and ignored when we wanted to suggest priorities of our own.
I knew that 2010 was going to be a disaster when the OFA people had meetings where they presented charts and graphs and lists of microconstituencies that benefited from particular programs. There was not even a single mention of values or messaging, whereas the 2008 campaign had been heavily values-based. I quit going to those meetings, and did as much canvassing as I had time for on my own, given that I was also organizing against the Catfood Commission. I got a lot of very good response to mobilizing people against that, from Democrats, Republicans and independents alike. Given that caucus states tend to have much stronger local party organizations, WA State resisted the red tide. Still, I could have done much more without the Obama-imposed distraction of the Catfood Commission.
And here we are at 2012 almost, and not a single word from OFA other than that "we have to educate people about Obama's accomplishments." Actually we shouldn't be doing anything of the sort, despite the fact that much useful stuff has gotten done. Why? BECAUSE THE GENERAL PUBLIC DOES NOT GIVE A BLOODY GODDAM ABOUT LAUNDRY LISTS! They care what is going on in their lives and about values, and no one can tell me what Obama's values are, except they seem to have something to do with government not being able to create jobs, regulations being bad and tax cuts being good.
The economy is still going straight to hell for the majority. This majority would still be strongly behind Obama if they felt he was on their side, no matter how bad things get. I don't feel that at all, and am working hard trying to convince all the 2008 PCO dropouts in my legislative district that we have to get more progressive people in locally and at the state level before we can change anything at the national level in any meaningful way. I'm having some success passing the word on what Republicans plan to do to Social Security and Medicare. I'm into politics for the long haul, but I'm part of a shrinking minority.
Profile Information
Gender: FemaleHometown: Washington state
Home country: USA
Current location: Directly above the center of the earth
Member since: Sat Aug 16, 2003, 02:52 AM
Number of posts: 51,907